This afternoon I submitted a meeting request to the Office of Information and Regulatory Affairs in the Executive Office of the President to discuss TSA’s unconstitutional program of singling out transgender travelers for extra scrutiny and abuse based on cissexist assumptions about anatomy. PDF available.
The Honorable Howard Shelanski
Administrator
Office of Information and Regulatory Affairs
Office of Management and Budget
Washington, D.C. 20503
Re: RIN 1652-AA67 – Passenger Screening Using Advanced Imaging Technology
Dear Administrator Shelanski:
As a transgender woman who occasionally flies for work and personal affairs, I have grave concerns with the draft final rule submitted to the Office of Information and Regulatory Affairs from the Transportation Security Administration on November 19, 2015. Put succinctly, the Advanced Imaging Technology (AIT) scanners unconstitutionally place undue scrutiny on transgender travelers because of cissexist assumptions about anatomy. Rather than being an occasional flaw in the system, the harassment of transgender travelers by TSA is designed into the system from the bottom up.
As you may be aware, the scanner is designed with a simple interface. An example, provided by the Department of Homeland Security,[1] appears below.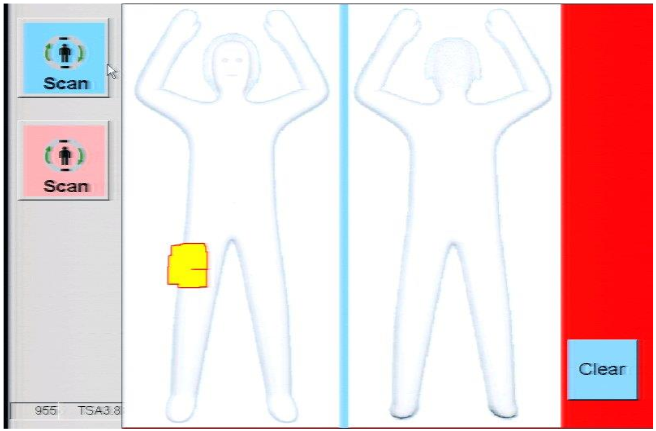
The scanner requires that a TSA employee press a pink or blue button, corresponding to the perceived gender expression of the traveler to be scanned. The traveler has no opportunity to ensure that they have been “read” correctly in a manner consistent with their gender identity and anatomy; they must hope that the TSA agent correctly discerns these things. This process is arbitrary, mistake-prone, and places an unconstitutional burden on transgender travelers to dress in a manner most likely to elicit a correct button press by government agents.
Once the button has been pressed, the AIT scanner is calibrated for certain anatomical assumptions. These assumptions are cissexist and fail to account for the existence of transgender bodies. If the agent presses the blue button, the AIT scanner assumes that the traveler will have a penis and no breasts. If the agent presses the pink button, the AIT scanner assumes the traveler will not have a penis but will have breasts. These assumptions are based in the cissexist logic that all men have penises and no women do, and similarly that no men have breasts and all women do. This logic is factually incorrect and places an unconstitutional burden on transgender travelers to explain their anatomy to uncaring government agents.
To solve this problem, TSA has proposed changing the word used for when the scanner detects something it was not programmed for from “anomaly” to “alarm.”
Meanwhile, TSA has also implemented a new policy for AIT scanner use. Under prior policy, any person had the ability to opt-out of the AIT scanner and be scanned physically. Many transgender travelers did so, rightly anticipating problems if they were to use the AIT scanner; while Ms. Shadi Petosky’s experience may be the most well-publicized,[2] she is far from alone in experiencing hellacious treatment by government agents for simply attempting to travel while transgender. Under the new policy announced on December 18, 2015, “TSA may direct mandatory AIT screening for some passengers.”[3] Now, not only is AIT screening the default, but it is mandatory for “some” passengers, with no indication of how this new authority will be used. Given TSA’s history of harassing transgender travelers, we are justified in being concerned.
If TSA wishes to maintain its AIT screening program, it must update the screening software and hardware so that is no longer based on government agents guessing the gender of travelers and so that it no longer assumes that all bodies are cisgender. Furthermore, while the AIT scanners continue to impose these unconstitutional burdens on transgender travelers, all travelers must have an unquestioned right to opt-out of the AIT scanner in favor of a physical screening.
I look forward to discussing this issue with your staff.
Sincerely,
Emily T. Prince, Esq.
[1] Department of Homeland Security, “Privacy Impact Assessment Update for TSA Advanced Imaging Technology,” DHS/TSA/PIA-032(d), Dec. 18, 2015, http://www.dhs.gov/sites/default/files/publications/privacy-tsa-pia-32-d-ait.pdf.
[2] See http://www.advocate.com/transgender/2015/9/22/one-trans-womans-tsa-horror-story, http://www.salon.com/2015/09/22/shadi_petosky_was_detained_by_tsa_for_traveling_while_trans_the_police_at_the_tsa_gate_were_awful_one_was_laughing_at_me/, http://www.nbcnews.com/news/us-news/transgender-woman-says-she-was-delayed-tsa-anatomical-anomaly-n431326, http://www.newsweek.com/shadi-petosky-transgender-woman-alleges-unfair-screening-tsa-orlando-airport-375220, http://www.nytimes.com/2015/09/23/us/shadi-petosky-tsa-transgender.html?_r=0.
[3] “Privacy Impact Assessment Update for TSA Advanced Imaging Technology”, supra note 1.